Day +1
Aside from 3am obs I slept surprisingly well – fitful dreams but nothing like the chemo delirium earlier this week when I spent a whole night dreaming I was Kamala Harris’s chief of staff in the run up to the US election – as if I didn’t have enough to do at the moment!
The whirr of the aircon in my sealed room overlooking the Royal Melbourne Hospital reminds me of being on a plane and all those trips to London for my last clinical trial – have I said how immensely grateful I am to be having this here?
I’ve always loved a test and on Monday I saw the Neurologist Fellow Dr Roberts Akhtvar who put me through an hour of cognitive testing…think Mensa meets Countdown for my UK friends and pick a word for the Australian ones – “I’ll have a P please Bob”. Here’s a sample of the kind of test I was put through.
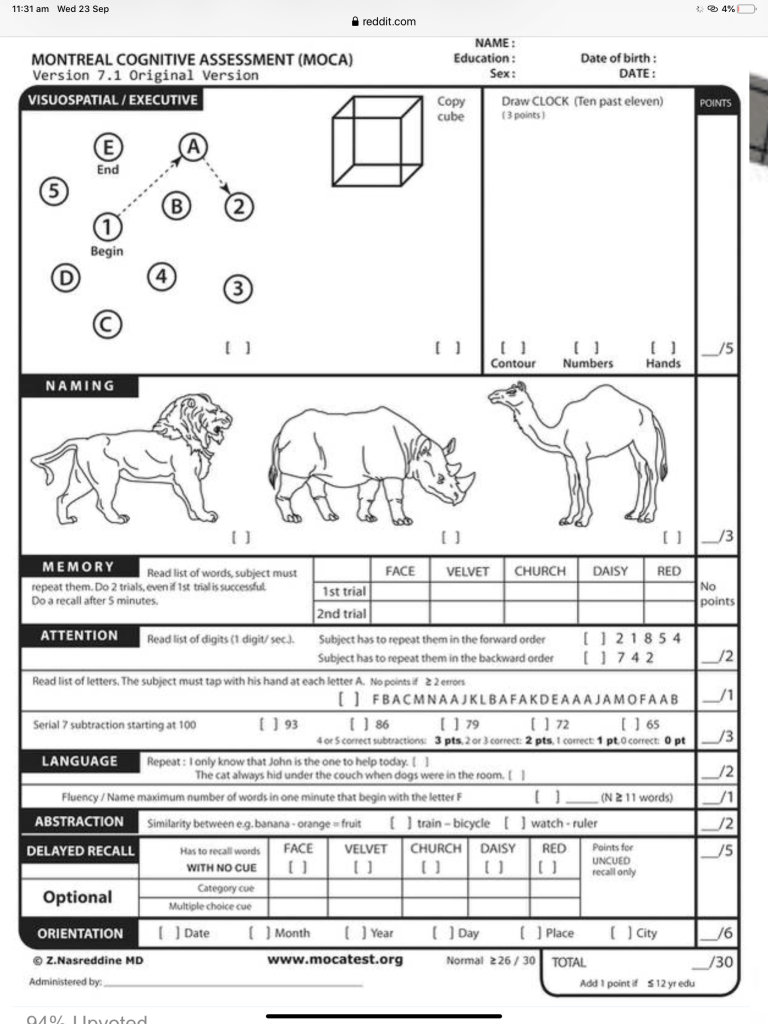
And more can be found here if you’re a glutton for punishment (with a note to my Mum not to try these herself):
https://www.dementiacarecentral.com/alzheimers-online-test/#mini-cog
The reason being there is very little data on the long term effects of neurotoxicity in CAR-T. This week data was published by the University Pennsylvania explaining why this neurotoxicity happens even in patients with very little disease. The CAR is programmed to target CD19 and there is a small population of cells expressing that antigen in the blood brain barrier. For science boffs here is that paper:
When the consultants did their rounds this morning I got to meet Mary Ann Anderson whose impressive body of published work I have read in full over the past few years but whom I have actually never met. She is one of the leading investigators into venetoclax resistance and I saw her initial data being presented at ASH in 2017 which is when I became aware that venetoclax might not be my cure. I’m pretty sure I’ve donated cells to her lab at the WEHI too.
Dr Anderson discussed the news to me that my latest testing showed that I have now developed 2 other chromosomal abnormalities which means my already poor prognosis disease is evolving which is possibly why it became resistant to venetoclax and may well become resistant to ibrutinib in the not too distant future (my words not hers). All that with the real risk of Richters hanging over me (a transformation to Diffuse Large B-Cell Lymphoma which is aggressive and very difficult to treat).
I really anguished over the decision to have CAR-T at this time. There is very little long term data as to what happens to patients who relapse on venetoclax and how long subsequent therapies will last. One of the most recent papers was actually published by the Peter Mac and again Dr Anderson is one of the lead authors along with the doctor looking after me on the ward this week Dr Thomas Lew – remember the name – the force is strong with this one…I took a photo of us but I’m sure this won’t be the last time I see him (hopefully this is my cure and the next time will be at a haematology conference rather than being his patient!).

Here is that paper which is also co-authored by my own doctor and one of Australia’s leading internationally recognised CLL specialists Professor Constantine Tam who called in to see me before he went off to clinic
See how seriously good my team is here in Melbourne?!
The fact is I had a very deep response to venetoclax and ibrutinib also gave me a deep response but I couldn’t run the risk of relapsing on drug again and not having another good option to jump to. The worst time to have an allogeneic stem cell transplant is as salvage treatment and I get bulky disease so getting that under control could be difficult. I know CAR-T is very new and cutting edge but I fancied my chances with this treatment much more than with transplant. And having it first doesn’t rule out that as an option in the future.
In an ideal world I would have been able to stay on ibrutinib for the next couple of years and the kids would be even older before I went for a curative, but more dangerous option. But there is little chance that there would be a CAR-T trial at my local hospital for CLL that will be open to me at just the right time and it’s unlikely it will be approved and funded for treatment by the time I need it so the only way I could get CAR-T was to act now – as Brian Koffman says we have to make decisions on the basis of imperfect information and this would never have been an easy decision to make.
I’ve been feeling that for the first time in my life I have been truly brave but have also feared I was being somewhat reckless with my good health – getting the results today which showed my disease is quickly turning into something that will become untreatable (what a smart cancer it is) makes that decision the right one. Now let’s see if CAR-T can work its magic. I’ll know in as little as 28 days.
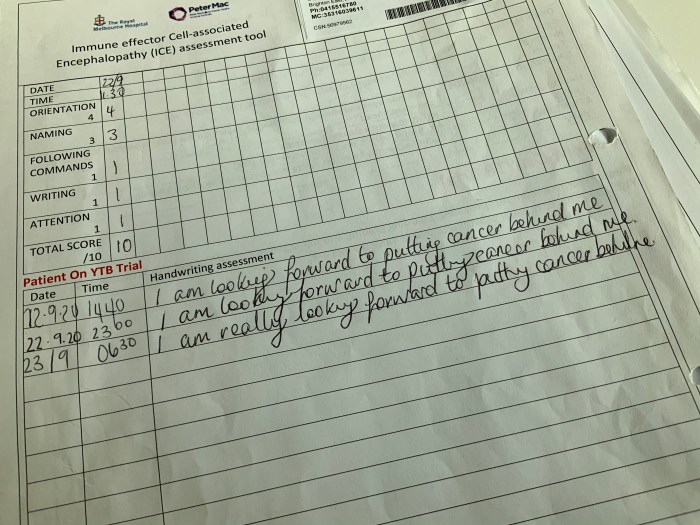
But back to the brain stuff – now as part of my program of routine observations I’m doing an ICE assessment (that stands for Immune effector Cell-associated Encephalopahy). Here’s the sheet for that – one of the first signs is deteriorating handwriting.
Dr Roberts Akhter from the Royal Melbourne Hospital also has me doing this iPad app test he uses to help track cognition in MS patients. You can find it on the AppStore by looking up Biogen CogEval – it only works on iPads (and not mini iPads for some reason)

What I like about it is it gives me some control and reassurance outside the obs periods – I truly do feel a bit like a ticking time bomb and when I get a score just by doing this 2 minute speed test which is in my normal range it comforts me. And I have a sheet of paper to note the time I did the score and my result so that data can be tracked. And there’s a lot to this – I am, if you hadn’t noticed, a bit of a type A control freak – I can’t help it, I’m the eldest of 5 girls and it’s just built into me. I’ve given up control in treatment before – we have to but it’s always been driven by the data (as the Victorian Premier would say, seriously Kamala Harris now quoting Daniel Andrews – what is happening to me?!). There is no data with this version of CAR-T though, as Mary Ann Anderson said to me this morning, minus the Darth Vader style heavy breathing, “you are the data”. I really have had to put my life into the hands of hundreds of brilliant scientists on the other side of the world and my excellent doctors here. As that syringe was gently squeezed into me yesterday I was just hoping no one was having an off day when my cells were made, that they’re perfect and my genetic modification lets me be Captain America instead of the Incredible Hulk.

And my friend Charlie Grieve from Brandcast Media just had a chat with me on Zoom from London which we recorded and he sent me this cartoon. I may start “vlogging” but let’s see how the next few days go but if anyone wants to see how little I’ve been impacted 24 hours apart from the bags under my eyes and Covid lockdown hair here’s that recording for posterity -I hope it gives some reassurance to others making this decision with the caveat that it’s early days and everyone’s disease is different but I know this would have helped me over the past two weeks as I counted down to Day Zero and I feel far better now than I did having the lymphodepleting chemo last week.














 The usual bloods were taken to be sent to Ohio and Livingstone in Scotland (everything locally came back completely in the normal range) and then I went off to clinic to see Professor Gribben. The hospital was in the middle of an IT crisis thanks to the hacking of their systems by some imbecile which was affecting their ability to order treatment for patients. I would imagine it has almost certainly cost lives, thankfully John had ordered mine the day before. He introduced me to another patient on the trial, Corin, who is also doing really well and is younger like me but more heavily pretreated and has been living with the disease for ten years, having been diagnosed at 38 with young children. It’s the first time I’ve met someone in such a similar situation and we managed to squeeze in a coffee before I left for New York the following day.
The usual bloods were taken to be sent to Ohio and Livingstone in Scotland (everything locally came back completely in the normal range) and then I went off to clinic to see Professor Gribben. The hospital was in the middle of an IT crisis thanks to the hacking of their systems by some imbecile which was affecting their ability to order treatment for patients. I would imagine it has almost certainly cost lives, thankfully John had ordered mine the day before. He introduced me to another patient on the trial, Corin, who is also doing really well and is younger like me but more heavily pretreated and has been living with the disease for ten years, having been diagnosed at 38 with young children. It’s the first time I’ve met someone in such a similar situation and we managed to squeeze in a coffee before I left for New York the following day.