I’ve now finished the 1st cycle of Obinutuzimab – they do choose some strange names for these drugs, ABT-199 is now called Venetoclax and referred to as VEN for short in the scientific papers, George Lucas eat your heart out.
I had another 1,000mgs on day 8 and another 1,000 yesterday on day 15. Side effects were minimal. The steroids on day 2 made me sweat a disgusting sweetcorn smell for a few days and I was relieved when they dropped those for days 8 and 15 and the anti-emetic made my bowels stop working – TMI? (I’ve been told I should enjoy that given how active they’ll be when I start the ABT-199). Yesterday I got away with having the Obinutuzimab on its own with no ‘roids or anti-nausea drugs and boy do I love the piriton appetiser – really relaxing, wish I could start every day with an infusion of that.
So now that I’ve officially been debulked how am I doing? Well first of all pictures tell a 1,000 words so let me show you how I have no visible lymphadenopathy left.

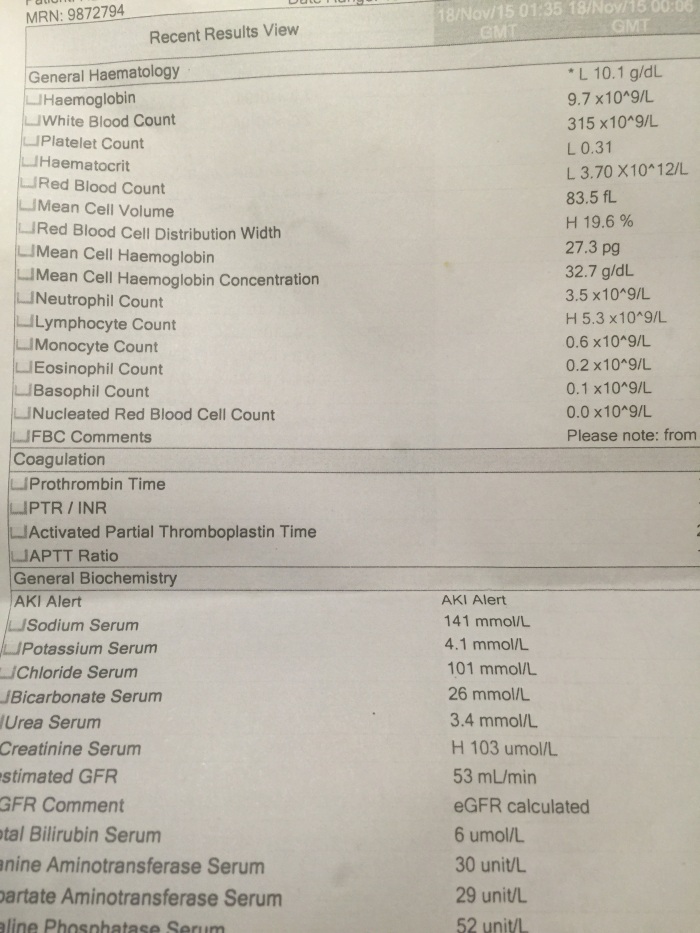
I had a full examination today and there are still some palpable nodes in various spots but they are all less than 1cm which is a big relief. This is my latest blood test too.
Although I’ll be having another 4 cycles of the Obinutuzimab over the next 4 and a half months I feel like it’s probably done as much as it’s going to do on its own….and it’s now time to bring in the big guns of ABT-199 aka my new friend VEN (he sounds a little Swedish doesn’t he?). So let me tell you about this amazing drug which I’ve spent the past 18 months trying to access. It’s been a long time love affair and I have to say now that we’re about to consummate our relationship I’m starting to get the wobbles.
ABT-199 is the most exciting weapon in science’s new arsenal against CLL (and several other blood cancers for that matter). For the geeks such as myself you should know that it targets a protein called BCL-2 which is over expressed in these cancer cells – by entering the cells and shutting this off it causes them to die and the effect is almost instantaneous.
Within hours of popping the pill it goes to work and cancer dies in massive amounts (apoptosis is the official term). The exciting thing is that, unlike chemotherapy, it is targeted therapy so the side effects are much more palatable. All but one that is. Sadly in early phase 1 trials of the drug (and we really are still in early trials – I’m in phase 1b) the immediate impact that it can have on the cancer cells wasn’t fully appreciated and at least 2 patients died in the US of what is called Tumour Lysis Syndrome. I heard that there was a third death in Australia but I haven’t read this in any of the published data. Tumour Lysis is where the body can’t process the amount of dead cancer cells quickly enough and it leads to kidney and ultimately heart failure.
Shockingly two patients died within hours of a dose escalation and, for as long as others like me enter these trials and others later benefit from this amazing drug, they will be constantly in our thoughts. We lab rats who enter Phase 1 trials are brave but we’re also very sick and have run out of options and this is the only way we can access cutting edge therapies.
I knew one of the patients who died via the CLL forum, a man called Randy Shirley who was not much older than me, with a wife and children and a zest for life who also blogged his journey and had been a huge advocate for other patients. He was interviewed by Andrew Schorr on Patient Power shortly before his death and Andrew, the beneficiary of a clinical trial himself, paid this tribute to him
Randy was at a centre of excellence for leukaemia trials in the US. His last post was a photo of the 12 pills he was about to take for his dose escalation along with the comment that he was the first patient to ever take such a massive dose. Within hours he had died at home and his death shocked the whole patient community. The trials were immediately suspended and the protocol changed to include more hydration, more hospitalisation and lower doses of the drug. While we mourned Randy, and my thoughts are still with his family, we were also scared that this might impede the approval of the drug which offers so much hope to those of us with this incurable disease. 53% of patients on one of the combination trials of ABT-199 with an older version of the monoclonal antibody Rituximab/Mabthera have no detectable cancer – that is an astonishing figure for a relapsed and refractory group of patients who were almost certainly facing death without this drug. Patients are going from hospices to being cancer free after this treatment and that’s unheard of in our disease.
Pharmaceutical companies need patients like Randy and myself to get their drugs approved but patients like us also need it to give us a chance at getting through this disease.
So, having said all that, Tumour Lysis Syndrome (TLS) is now my most immediate fear. Because I’ve been debulked and my White Blood Count is lower the danger shouldn’t be as great, but today I had a blood test which showed an elevated creatine level in my test from last night which is a warning sign for kidney damage. I am drinking so much water but have now stepped it up even more and my test from lunchtime today came back normal but it was a bit of a fright for me.
I will be admitted to the hospital on Monday afternoon for IV hydration overnight and will take the first VEN pill on Tuesday. They’re starting me off at 20mgs and I will take that daily for a week before I’m escalated to 50mgs for a week, then 100, 200 and finally onto my ongoing dose of 400 mgs a day. 2 hourly blood tests will follow and they’ll be particularly watching my potassium and creatine levels which is what tells them TLS is happening. My understanding is that the renal team will be on standby if I do start showing signs of this and they will quickly start flushing me out, I’m assuming with dialysis, to help process the drug and dead cancer out of my system.
It’s all a little scary and I know, having travelled around the world to meet my new love, I’ll be a lot happier when I know the only thing he’s going to kill is my cancer. Sometimes knowing too much is a bad thing but that’s what informed consent is all about.

hope all goes well Deborah xxx
LikeLike
Thanks Mrs Heaver! x
LikeLike
Hi Deb,
What a wonderful and enlightening summary for my uneducated mind and limited knowledge of this area.
I wish you well and look forward to reading about your positive progress.
Cheers Keith x
LikeLike
Thanks Keith – the haematologist I saw today asked if I was medically trained and I said sadly not, just an educated patient with a lot of skin in the game!
LikeLike
You have become an honorary arm chair hematologist! That was such a beautfully done and courageous summary with your *not* TMI details Deb! Your neck looks simply swan-like as you would say. You are in great hands and that nice and easy VEN ramp up will be just what the doc ordered. We are cheering for you.
Wup
LikeLike
Thanks whatsupdoc – I do think this combination will do the job – love that Dr Kipps latest discussion on novel therapies mentions these two drugs first…I just hope everyone will be able to access them and that patients like me can help establish the safest way to administer the protocol.
LikeLike
I’m not surprised he thought you were a medic – your analysis is so forensic! Love, hugs and lots of positive vibes to you xxx
LikeLiked by 1 person
Looking forward to getting back to my none medical life though Sam – thanks for the good vibes, hope you and yours are well xxx
LikeLike
Hi Deb,
Wishing you all the best for Monday – I will be thinking of you.
Greg
LikeLike
Thanks Greg – check out the ABT-199 plus Ibrutinib trial at the Peter Mac – great results under Constantine Tam for MCL – hoping it will open for CLL soon.
LikeLike
Very best wishes for the treatment. You are right that we owe a great debt to those who have gone before us in clinical trials.
LikeLike
Thanks Graham! Best wishes to you too. Deborah
LikeLike
Darling, you are such a positive person and have waited patiently for ABT or rather Ven. This trial has never just been about you singuarly, but about trially a drug that you have faith in that will aid those who are fighting a battle every day. Love you so much xx
LikeLike
Not that your biased! Thanks Mum, love you too x
LikeLike
Hi Deb
This is Dave from across the pond at OSU, on the same trial, but adding ibrutinib to the cocktail. You mention the creatine level, I always wondered why I was visited in my room from the kidney Dr., now I know. I’m taking Allopurinal to help with the kidneys, are you? I’ve had flow tests to see how the drug is working(see cll forum for results), are you going to have them? My main concern is they are stopping at 100mg of abt, I would like to go high if its needed(the heavy lifting is already gone in the trial). Best of luck, and “MY THE FORCE BE WITH YOU”
Dave
LikeLike
Thanks Dave – I just heard word that Ibrutinib plus ABT-199 has put an MCL patient, the first in Australia to enter the trial, into an MRD- remission and he was very ill before, so I’m very optimistic about your combination. Yes I’m taking 300mg allopurinol daily along with acyclivor (to prevent shingles, haven’t had this but don’t want it either!). I’m excited about your flow tests, I asked about these but they won’t do them until at least month 4 (I’m still in month 1). I agree that I’d want a higher dose of ABT (I’m going up to 400mg) but I imagine they need to be cautious given you’re going for the triple whammy of obinutuzimab, ABT plus Ibrutinib – can’t even imagine what that combo will cost when it comes to market! We are so lucky to be on these trials. Loving your results! Deb x
LikeLike
Please post the flow results, starting with the base line, so we can compare. MRD- here we come
Dave
LikeLiked by 1 person
Will do – I think my baseline was worse than yours – see I’m so competitive – race you to no detectable disease mate x
LikeLike
Wow this is my favourite blog so far. So much information to take in, brilliantly explained. You are too smart for your own good! Excited for you to finally get this wonder drug into your system so you can tuck this inconvenient chapter of your life far away and move on stronger than ever. Love you so much big sis xxxx
LikeLike
Thanks Emily, looking forward to a boring week! Love you too x
LikeLike
Deb
How did your 20mg dose of ABT 199 go? Did your potassium show some increase? I had 4 hour draws for the first 12 hrs.(if its the same for you, good luck in trying to get some sleep tonight)
Dave
LikeLike
Yes mine were 2 hour blood draws! So so tired x
LikeLike